|
The most common type of cancer of the tongue is called Squamous Cell Carcinoma. There are other types of cancers of the tongue but they are statistically uncommon. If you have questions about some of these more rare cancers, read more.
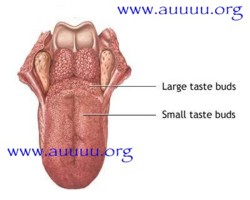
The tongue is actually divided into 2 separate anatomical areas, the oral tongue is the part you can "stick out" at somebody and extends backward to a V-shaped group of lumps on the back of the tongue which are actually specialized taste buds. The base of tongue is behind these. The oral tongue and the base of the tongue comprise the whole tongue but it is important to know that they develop from different embryonic tissue and really are somewhat dissimilar. Most importantly, this explains why the treatment for squamous cell carcinoma for the oral tongue is usually quite different from the treatment for squamous cell carcinoma of the base of tongue.
Squamous Cell Cancer of the oral tongue
This tumor is usually located on the side, or what we call the lateral border, of the oral tongue. It is usually somewhat ulcerated and is grayish-pink to red in color. It will often bleed easily if bitten or touched. It is generally seen in the older age groups though we have had one 21 year old woman present with a small cancer, and just recently a 32 old lady from the Austin area come to us from the Internet for treatment of a significant squamous cell cancer of the tongue. Smoking and drinking are known to contribute to the formation of the cancers, although some folks have developed squamous cancer of the tongue with no known extra risk factors.
Most very small cancers of the oral tongue can be quickly and successfully treated by surgical removal leaving behind little cosmetic or functional change. THIS IS NOT ALWAYS TRUE, HOWEVER, AS THERE CAN BE MANY VARIABLES AND FACTORS THAT CAN SERIOUSLY IMPACT SPEECH AND SWALLOWING. This can only be assessed by a face to face Surgeon/Patient meeting and examination.
Larger cancers may indeed have some effect on speech and on swallowing, but one must remember that not treating this problem would cause far more significant problems, up to, and including death. If one thinks about that for a moment; a few changes in speech or swallowing seem like a pretty good swap.
There is a school of thought that small oral tongue cancers can be better managed by radiation therapy alone, and this is indeed true in some cases, especially where the patient has serious heart and/or lung disease that might make anesthesia risky. Fortunately, this is a rare occurrence.
The main reason for treating small sqamous cancer of the oral tongue with surgery is that it is at least as curative as radiation, possibly better, it is over with quickly, oftentimes done as an out patient procedure instead of 5 - 6 weeks of daily therapy, it may be significantly less expensive, and finally, and most importantly, it means that if a patient were to later present with a 2nd or 3rd Squamous Cell Cancer of the mouth/throat/or voice box area, you would still have radiation therapy as a treatment option, perhaps then being able to avoid a significant and disfiguring operation. There is a limit as to how much radiation normal tissue can take before it dies.
Some cases of Oral Tongue Cancer can be treated with just removal of the primary tumor in the tongue. But as the size of the primary tumor increases the statistical possibility of some cancer cells spreading through lymphatic vessels to the lymph nodes of the neck increases. The site and pattern of the involved lymph nodes is pretty much constant --- that is to say we know where in the neck to look for enlarged lymph nodes that might contain metastatic cancer cells from the oral tongue cancer. Exceptions to these rules are sometimes seen, but they are uncommon. When the presence of enlarged lymph nodes in the neck is detected or when the index of suspicion is high that there may be cancer cells present in lymph nodes, then an operation called a neck dissection is performed to remove these "secondary" deposits of cancer. Remember, the oral tongue cancer is the "primary" tumor from where the spreading cells originate.
There are many forms of neck dissections from radical to conservative and I can not really go into the differences and unique characteristics of each one. Suffice to say that this is an area of medical judgement and decision making that relies heavily on the experience of the surgeon. While many physicians may have had some exposure to neck dissections at some point in their career, there are very few Head and Neck Surgeons, usually found in large medical centers, who can truly say that their career has been dedicated to this type of disease and they have done hundreds or perhaps thousands of these procedures. At The Head and Neck Surgery Clinic of Houston, we will have been doing Head and Neck cancer surgery and neck dissections for half a century come 1999.
Finally, there may sometimes be the need to perform plastic surgery and/or reconstruction following removal of the tumor, and radiation treatments may have to be given after the surgery to try to minimize the possibility of recurrence of the disease and ultimate treatment failure. Yes, sometimes in spite of every effort, every bit of hard work, in spite of supportive care and even our prayers, some patients will be lost to this disease. It is a sad thing to have to watch and be a part of, but it is one of life's unpleasant realities. For now, we will have to content ourselves with the knowledge that most of our tongue cancer patients survive quite nicely and hope that new research and new discoveries in the future will allow us to help our patients even more.
Squamous Cell Cancer of the base of tongue
Like the oral tongue, the base of tongue (or posterior 1/3) can also grow several types of cancers, but again, squamous cell carcinoma is the most common and we will direct our comments with that in mind.Unlike oral tongue cancers, base of tongue squamous cell cancer is usually larger when diagnosed because in the early stages it can not be seen and it creates few, if any, symptoms. Later however, base of tongue cancer may create pain, a sense of fullness, changes in what the voice sounds like, and perhaps even some difficulty in swallowing. Also, because the diagnosis often comes a bit later, a greater number of patients with this disease will already have neck metastasis, that is, cancer cells in the lymph nodes of the neck, by the time they are seen by the Head and Neck Surgeon.
While it may technically feasible to surgically remove some base of tongue cancers, it is our opinion that most can and should be treated by radiotherapy. These tumors are arguably more sensitive to radiation treatment than some other cancers. Certainly, there are exceptions to this. Radiation therapy can also be used to control the cancer in the neck nodes as long as it is not too advanced. Interestingly, in those cases, we will sometimes remove massive neck node disease before starting radiation therapy when we know that x-ray therapy alone would not be successful in controlling the neck disease.
The prognosis after treatment of base of tongue cancer will vary from patient to patient as with any type of malignant disease. It has been our experience that the cure rate is good, but not quite as good as for early detected oral tongue cancer. The fact that base of tongue cancers are usually larger at the time of diagnosis probably is a significant contributing factor to this disparity. Very large base of tongue cancer may require a combination of surgery and radiation.
|